Published On Sep 7, 2009
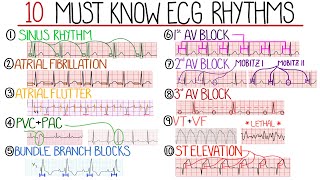
The most common cause of a lethal dysrhythmia is by a PVC hitting the peak of the T wave (known as R-on-T Phenomenon). This causes a pulseless shockable or non-shockable rhythm in at risk patients. 90% of cardiac arrests in adults are shockable (Pulseless VTach/Ventricular Fibrillation). This rhythm started with multifocal PVCs to a wide complex tachycardia (Pulseless VTach). This can only last from a few seconds to a few minutes before it becomes Coarse Ventricular Fibrillation (if no CPR and Defibrillatory shocks were administered). Coarse VFib can only last for about 4-5 minutes before it becomes Fine VFib. From then on, you have seconds for Fine VF to become Asystole.
INTERVENTIONS: Based on AHA 2016 Guidelines
For VF/pVT:
High quality CPR
Defibrillate 120-200 J biphasic or 360 J monophasic every two minutes
Give Epinephrine 1 mg every 3-5 minutes, followed by a 10-20 mL flush of NS/LR
May give Amiodarone 300 mg IV/IO bolus if refractory (if patient is not hypokalemic)
May give Lidocaine 1-1.5 mg/kg IV/IO bolus if refractory (if patient is hypokalemic)
For Asystole/PEA:
High quality CPR
Give Epinephrine 1 mg every 3-5 minutes, followed by a flush of 10-20 mL NS/LR
Correct possible causes (H/Ts)
Possible causes:
Hypoxemia
Hypo/Hyperkalemia
Hydrogen Ions (Acidosis)
Hypothermia
Toxins
Tamponade, Cardiac
Tension Pneumothorax
Thrombosis, Pulmonary Embolism
Thrombosis, Acute Coronary Syndrome
If ROSC (Return of Spontaneous Circulation)
1. Optimize ventilation and Oxygenation
Advance airway placement
Ventilate 10-12/min
Keep O2Sat greater than 94-99%, PETCO2 35-40 mm Hg
2. Treat Hypotension: Keep SBP above 90 mm Hg
Give 1-2 L NS/LR
May administer Dopamine 5-10 mcg/kg per minute IV/IO
May administer Epinephrine 0.1-0.5 mcg/kg per minute IV/IO
Treat H/Ts
12-Lead ECG
3. Consider TTM (Targeted Temperature Management) if ALOC
Give cold NS/LR 4°C to reach a core temp of 32-36°C for at least 24 hours or greater
Other cooling measures are used to induce hypothermia (jell beds/pads, thermo-coolers, cooling blankets, etc)
CONSIDERING CODE TERMINATION:
Unsafe scene
If (central) rigor mortis exists. Patient's intercostal muscles already filled with lactic acid from prolonged CPR disallowing compressions and decompressions
If DNR (do not resuscitate). It's obvious you don't start ACLS when you have the DNR papers on chart. This happens sometimes when the patient arrives in the ER first via ambulance and the family coming from somewhere else arrives with the DNR papers.
MD orders
Code Team decision
Lividity
Decapitation
Family request