Published On Jan 24, 2024
App: TruMonitor
Music: Deep Sea Orchestra - Aalborg Fantasy Soundtracks
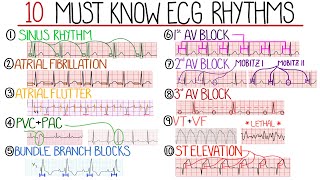
P waves are described as "Sharks Teeth," "Sawtooth," or "Picket Fences." T waves are not visible. Can also have 2:1, 3:1, or variable blocks. Atrial flutter occurs when an abnormal conduction circuit develops inside the atrium, allowing the atria to beat excessively fast, about 250-300 beats per minute. If the rate goes over 150 bpm, it can also be interpreted as SVT. (AVNRT).
CAUSES:
Decreased blood flow to the heart (ischemia) due to coronary heart disease, atherosclerosis, or a blood clot
High blood pressure (hypertension)
Disease of the heart muscle (cardiomyopathy)
Abnormalities of the heart valves (especially the mitral valve)
An abnormally enlarged chamber of the heart (hypertrophy)
After open heart surgery
Drugs (cocaine, methamphetamine, diet pills, etc.)
Chronic obstructive pulmonary disease
Alcohol (liquor, wine, beer)
INTERVENTION: If stable
Keep airway patent, support breathing
Keep O2Sat 94-99%, PETCO2 35-40 mm Hg
Start IV/IO, 12-Lead ECG, draw/send labs
NO Adenosine!
May give Sotolol 100 mg (1.5 mg/kg) IV over 5 minutes. Avoid if prolonged QT
May give Metoprolol 5 mg IV over 2-5 minutes, may repeat every 5 minutes. If there is no history of heart disease or CHF only.
May give Diltiazem 0.25 mg/kg IV slow over 2 minutes, may repeat every 15 minutes. Max. The dose is 0.35 mg/kg.
INTERVENTION: If Unstable
Consider sedation
If less than 48 hours onset: administer Synchronized Cardioversion 50-100 J
May administer B-blockers or Calcium-channel blockers (CCB)
Administer anticoagulants
If greater than 48 hours: give B-blockers or CCBs, anti-arrhythmics with anticoagulants only. NO cardioversion!
Other possible interventions:
Cardiac ablation
Anticoagulation
Rate controllers (B-blockers, CCBs, antiarrhythmics)
Implanted cardioverter-defibrillator
Based on AHA ACLS 2016 Guidelines